

Today’s PrimalMed Prescription…Consider BOTH sides!
Today’s PrimalMed Prescription…Consider BOTH sides!
If we agree that so much science is still unsettled, can we consider that sometimes, seemingly discordant views can BOTH be valid?


On January 10, 1976, the world was introduced to “New Shimmer.” What is or was New Shimmer and why am I choosing to lead this science heavy missive off with an obscure reference? Season 1, Episode 9 of Saturday Night Live ran a mock commercial on this revolutionary product that was non-dairy and came in a nozzle can. Behold, New Shimmer! While Gilda Radner and Dan Ackroyd argued over its merits as to whether it was a floor wax or a dessert topping, Chevy Chase came to the rescue with an all-knowing grin and assured us that New Shimmer was a floor wax AND a dessert topping. Tastes great and just look at that shine!
How can BOTH be right? How can two seemingly opposite narratives both be valid? Can we consider both sides?
In the same vein, people ask me all the time about STATINS and their current role as a lipid lowering medication. There are differing opinions re: the utility and relevance of statins in 2023. Are they still considered a life saving medication? Is the lipid hypothesis as a driver of cardiovascular disease still relevant? Can there be differing opinions and views on this topic that are both somewhat right with each having merit?
I say, “Please note that I am a curious radiologist with an interest in metabolic health and strategies to optimize health span. I am not a cardiologist so what follows is my opinion and DOES NOT constitute formal medical advice.” But, I am happy to opine.
Here’s the deal:
Statins are a pharmaceutical intervention that lowers serum cholesterol. Remember the “I’m down with Crestor!” commercial from a few years ago? Any AARP member who watches the evening news is no stranger to the never ending ads for the statins. They do lower the LDL-C number but do they extend lifespan in a statistically significant way that outweighs any side effects? Do they prevent initial events or are they more relevant in those that have already had a cardiac event?
Are the benefits from statins due to the fact that they lower a number, namely the LDL number on your blood panel or do they impart their efficacy by lowering inflammation at the level of the lining of the blood vessel?
The LDL hypothesis is just that, a hypothesis from almost 40 years ago. It states that LDL is the causative driver of ASCVD ( atherosclerotic cardiovascular disease) yet many patients with heart attacks and strokes have a normal or low LDL. What gives? Time to question the old dogma.
Many well respected lipidologists and cardiologists believe you can’t lower LDL enough, while many other respected physicians realize that LDL is a necessary molecule that transports cholesterol, a necessary precursor for steroid and sex hormone synthesis and cellular membrane architecture as well as having a role in Vitamin D production and energy transport. We NEED cholesterol.
There are some downstream effects that arise from using statins to block cholesterol synthesis in the liver. In about 5% of patients, side effects can include muscle weakness, abnormal liver function tests and in some, dysregulated glucose metabolism with an increased risk in developing Type 2 Diabetes.
So maybe in those folks, conventional statins are a no-go and a newer class of drugs is needed. They are called PCSK9 inhibitors like Repatha. They upregulate LDL receptors so they increase the clearance of LDL from the blood. In some studies, they decrease the risk of CV events in some sets of patients, especially those with a nasty genetic variant that causes an elevated Lp(a). Lp(a) is lipoprotein marker on your LDL that makes you at risk for increased clotting and CV events.
BUT WAIT…science marches on…
The latest literature says that maybe we shouldn’t focus on LDL cholesterol per se since it is a calculated number, but rather look at levels of a lipoprotein marker on the periphery of the LDL molecule called ApoB. This is a more nuanced approach and more directly measures the number of LDL particles in the blood rather than the calculated concentration of LDL. It’s a subtle difference but cardiologists believe that measuring ApoB is a better marker to calculate ones risk of a CV event. (Note to self: make sure to get ApoB measured next time in addition to the standard blood tests of LDL, Total Chol/HDL and Triglycerides).
Now let’s step back and get curious.
What if LDL or even ApoB doesn’t CAUSE heart attacks or strokes. Maybe they are somewhat involved in the cascade of events involved in the atherogenic process, but perhaps we can look UPSTREAM and see WHY it might be an issue at all. Why would we have these LDL transport molecules in the first place, that are needed to transport cholesterol throughout the blood if it was a prime driver of CV disease?
Is it time to consider another hypothesis?
Enter, the Thrombogenic hypothesis. This has been discussed in the last few years especially by Dr. Malcolm Kendrick, a Scottish cardiologist. In this hypothesis, the atherogenic plaque is not caused by LDL or ApoB but rather by a blood clotting cascade at the level of the inner lining of the blood vessel (the endothelium) that starts with inflammation and the intrusion of oxidized or damaged LDL particles.
One analogy compares the inner lining of your endothelium to a fence that borders your front yard. The street is your arteries. If you can keep your endothelium intact, then inflammatory cells and oxidized LDL particles (with the ApoB marker) can’t burrow into the vessel wall and start the process of forming blood clots and atherosclerotic plaque. The endothelium itself is lined with a coating called the GLYCOCALYX, that makes the inner lining smooth and slippery and not conducive to disruption and plaque formation.
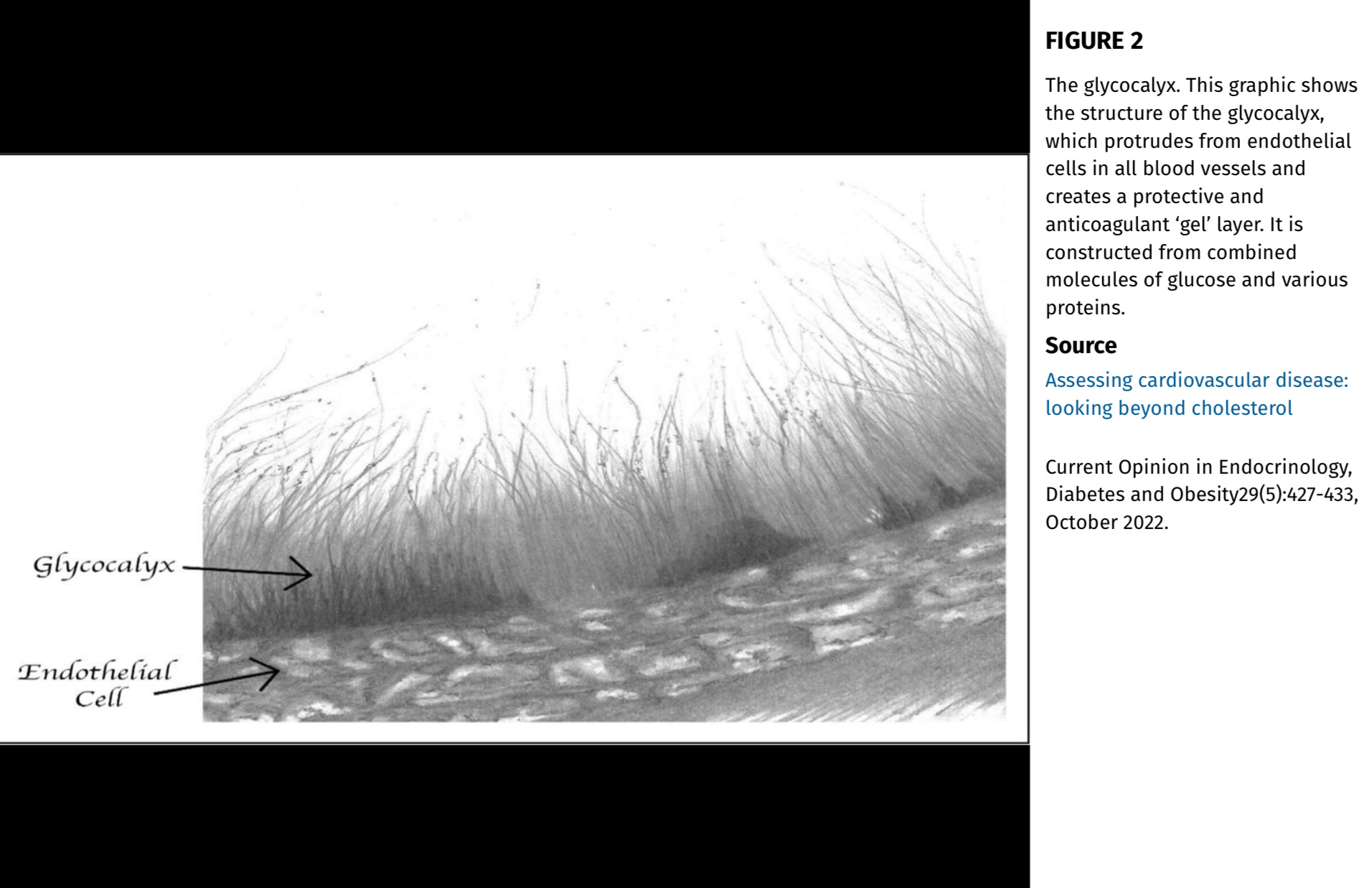
So, HOW do we preserve the glycocalyx and endothelium so that ApoB and LDL is not even a concern. Wouldn’t it be better to protect the fence from intruders so we would NOT need pharmaceutical intervention?
So which hypothesis is correct? One that supports the role for statins and PCSK9 inhibitors in select patients to drive down ApoB or one that focuses on preserving the integrity of the glycocalyx and endothelium first?
Maybe BOTH. I submit that the answer can be yes, no, or maybe depending on the individual patient. The whole topic of cholesterol and LDL is complex and nuanced. There is so much about personalized medicine we don’t yet know.
LDL and ApoB only become a particle of concern when they become oxidized and breach the compromised and damaged fence so:
DEFENSE, DEFENSE, DEFENSE!
Protect your fence. The best way to prevent endothelial damage is:
-Don’t smoke (that’s a direct chemical assault on the endothelium via toxic aldehyde metabolites. I assume most PrimalMed readers don’t smoke).
-Maintain a normal blood pressure. Hypertension is a source of a direct shearing mechanical force on the endothelium. Get your BP checked and get it down to normal levels. Increasing nitric oxide levels with exercise and resistance training help protect the endothelium. Diet and lifestyle modifications are key and yes, sometimes meds are indicated.
-Stay away from the SEED OILS. See prior posts. Oxidized PUFAS (polyunsaturated fatty acids) found in seed oils (Soybean, Corn, Canola, Sunflower etc) can cause damaging inflammation to the LDL molecule. Oxidized LDL are small and can penetrate the fence. The oxidized metabolites of these linoleic acids (OXLAMS) include aldehydes, similar to those found in the cigarette smoke, that directly damage the glycocalyx and endothelium, and in effect, damage the fence.
Another no-brainer is to limit excess added sugars and ultra processed garbage. No need to snack all day, since you don’t want to be living on a continuous insulin drip. The up and down spikes in glucose and insulin can be inflammatory. Inflammation can damage the fence.
What if the fence is ALREADY damaged and broken?
50% of Americans are obese or overweight. A fair amount are diabetic, pre-diabetic or insulin resistant. An estimated 93% have one or more of the components of Metabolic Syndrome (high fasting blood sugar, hypertension, central obesity, low HDL, high triglycerides). Many Americans still smoke. In these folks, the endothelium IS compromised and perhaps a statin is needed to help keep ApoB down and mitigate the atherogenic process. If you have already HAD a heart attack or have a stent, then you have a compromised endothelium, so perhaps statin therapy is indicated.
TL;DR
When approaching your cardiovascular health, stick to the big rocks or low hanging fruit (choose your metaphor) since the ever changing and often conflicting studies and science you read on Apple News and FB are usually statistically flawed or limited. The headlines are geared to grab eyeballs. Those “Do this or Don’t do this” articles are often biased.
What are the no-brainers?
Not smoking, normalizing blood pressure, fueling your body with adequate protein and getting up off the couch to maintain appropriate muscle mass are your non-negotiables. Walk after meals to keep those glucose spikes low. Throw in those PrimalMed pushups and squats!
For many years, the goal was simply to lower that LDL number. Now, many are looking at a more curated, personal approach by looking at ApoB, Lp(a) and LDL particle size and number, as well as now measuring oxidized LDL. We can do a lot more in 2023 than in 2003. I have been to conferences where many think that just looking at LDL as an isolated metric may be myopic, and they focus on lowering triglycerides, increasing HDL, lowering inflammatory markers such as C-reactive protein, and lowering fasting insulin levels, which are a key predicting marker of pre-diabetes and metabolic dysfunction.
See below: This is a commentary. I am not a fan of absolute conclusions and prefer to say “may or may not” be warranted. But it certainly is interesting and makes you think about new and changing narratives.
If you are on a medication such as a statin, under proper medical supervision, and feel fine with NO side effects, and it’s working for you, stay the course since there is still so much we DON”T yet know in the field of personalized medicine.
Remember the term “glycocalyx.” And focus on keeping your endothelium healthy. You can tell your kids you read about it in Your PrimalMed Prescription way back in 2023.
The great philosopher Sy Syms once said, “An educated consumer is our best customer.” That’s the goal of this post. Recognize that what works for one may not work for the other since a lot of the science, especially nutritional science is still not entirely known. A lot of our BEST ADVICE is still based on hypothesis. Stay curious.
And remember that opposing opinions can BOTH have merit.
New Shimmer CAN be a floor wax AND a dessert topping.
Today’s musical interlude? Well I hope you listened to it at the top of the post. But in case you miss the Go-Go’s and the smooth sultry sounds of Belinda Carlisle, here’s a newish cover of this classic.

Thanks for reading and sharing !!! Glad that the subject matter was easily digestible!!!
Great post and I actually understand the science this time!