

Today’s PrimalMed Prescription…think upstream!
Today’s PrimalMed Prescription…think upstream!
Creaky wonky knees? Look north to your glutes!


How’s this for a random intro?
A radiologist and an orthopedic surgeon get in a car and drive from LA to Vegas. We don’t walk in to a bar, but we do walk in to Barstow’s iconic diner, Peggy Sue’s, for some omelettes, coffee, and a healthy dose of 1950’s nostalgia. We are driving through the desert, listening to the Hollies sing about the road with its many a winding turn.
Given this apparent moment of zen, the conversation naturally turns to…you guessed it…the topic of knee pain and the value of using MRI to image those achy knees.
I’ll admit, I started the conversation. Why? Well last week I was reading MRIs at the hospital, and having always taken a keen interest in the musculoskeletal cases, I thought why not trade notes with one of SoCal’s finest surgeons? I had a captive audience for 4 hours!

Here’s a patient with knee pain. This guy is a middle aged athlete. “Everything was going just fine,” he says, “until OUT OF THE BLUE, doc, I went on a slow easy run and my knee started to ache and now it’s killing me!”
First of all, unless you are skiing and you fall and rupture your ACL, or playing football or soccer and get clipped and tear your MCL, most things just don’t happen ‘out of the blue.’ There’s usually a reason that caused your knee to be vulnerable to injury and pain.
My radiologic diagnosis? Sure I could eloquate about the specific anatomy and pathologies but I prefer to just call it an ‘angry knee.’ The MRI shows a lot of fluid/edema in and around the inner knee ligaments and tendons and degenerative changes in the medial meniscus cartilage that you may see in many adults over the age of 50.
Many folks will have abnormal findings on an MRI with little or no symptoms. Way before MRIs, there was this time honored clinical skill called the physical exam. As my esteemed Orthopedist friend opined, and I agreed; there is no substitute for a good physical exam by an experienced specialist. Torn ACL or MCL? Yeah, arthroscopic surgery may be in your future. An achy knee with some chronic pain without an acute injury? The MRI, if one is needed at all, is simply a tool that your doctor uses to figure out the proper treatment. Like starting with physical therapy or seeing a functional chiropractor.
Remember, just because we see something on an MRI or imaging study does not mean that THAT abnormality is the actual cause of your pain or instability. A good physician will treat the patient, not the image.
You can throw all the ice and anti-inflammatories at that knee, but that’s just a band-aid, right? We physicians can diagnose and treat…but the functional approach, THE PrimalMed approved approach, calls for figuring out how you got there in the first place. What led up to the swelling and pain? What’s the ROOT CAUSE? If you think it happened out of the blue, well, I suspect there were some tremors and rumblings in that knee long before that volcano erupted. Time to LOOK UPSTREAM.
At PrimalMed, we have said (and to paraphrase Hippocrates) that “All disease begins in the GUT.” Here’s today’s bromide…“Your leg aches and pains begin in the BUTT!”
That’s right! You got a wonky knee? Unless you fell down a flight of stairs and twisted your knee or got taken out by a linebacker, I submit that it is your UPSTREAM muscular weakness and imbalance (that places excessive stress on the knee) that is the root cause of your ‘out of the blue’ wonky knee. Do you sit a lot? Your glutes and hips take a siesta (sleepy butt syndrome) and become dysfunctional. They can’t support your athletic pursuits. Take care of the upstream and then and only then can you assess the DOWNSTREAM kinetic chain.
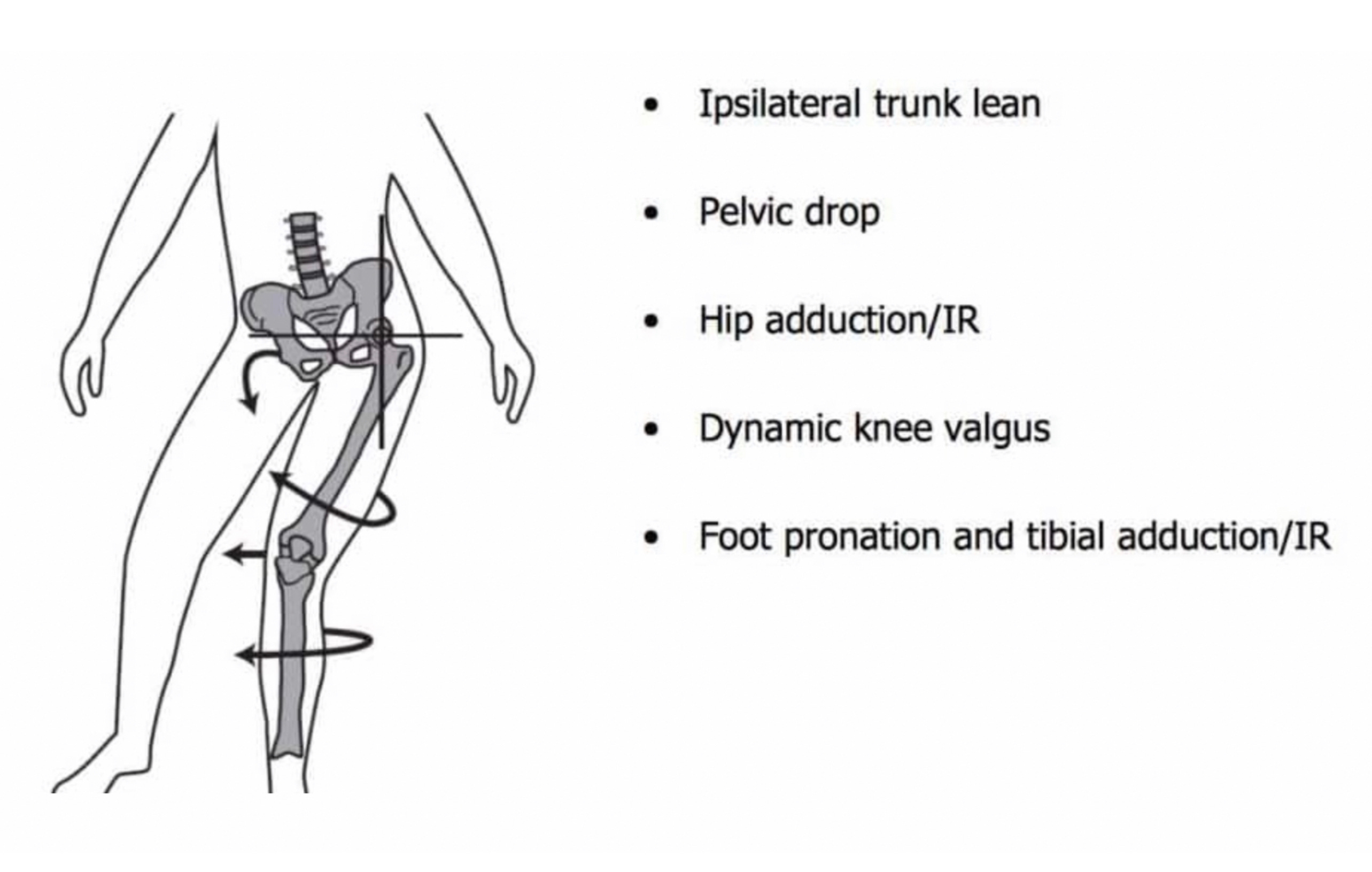
Weak glutes and hips means your pelvis is unstable, and when you run, your hip drops and your thigh and shin bones torque and rotate to support you. That puts undue stress on your knee. No bueno. Wonky knee alert!
Runners in particular have a malady reserved just for them! It is called Patellofemoral Pain Syndrome or Runner’s Knee. Your patella or knee cap slides side to side when you run because the supporting muscles that are supposed to ensure that the patella tracks straight and smooth are too darn weak.
In this case, a muscle called the VMO or your inner quad is too weak and your iliotibial band and outer quad muscles are too tight. Quick fix here for you runners. Roll out the muscles leading to your IT band with a foam roller. Go slow and start with a SOFT foam roller and target the Vastus lateralis, NOT the actual IT band near the knee. See below diagram. Stay off the tender knee!
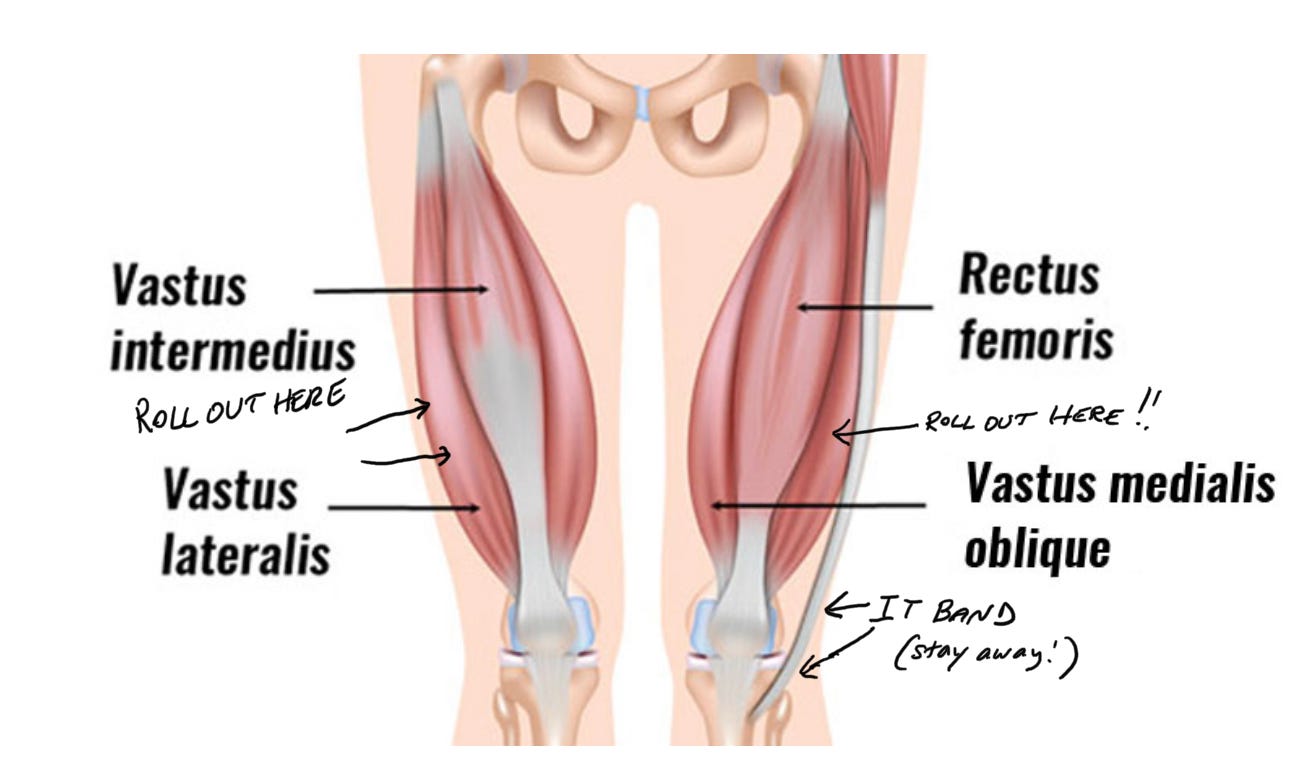
The IT Band is TOO tight and tugs on the patella. Remember, DO NOT stretch an injured tight muscle. Roll it out. You’ll feel some sore spots or knots. Those are called TRIGGER POINTS. You may feel them in the Vastus medialis and Vastus lateralis. Roll and massage to release those tight knots. If you are curious, grab a copy of the classic tome by Claire Davies, ‘The Trigger Point Therapy Workbook.’ You’re welcome.
Strengthen your VMO. It is too weak and can’t stabilize your patella. Over time, you get wear and tear on the underlying patellar cartilage and BAM, runners 🏃♂️ knee strikes again. Leg lifts and Wall sits. Look those up online. Your quads will thank you.
TL;DR time!
Nothing happens ‘Out of the Blue!’
Look to the upstream to fix the downstream! Respect the kinetic chain! Achy breaky knees start with weak butt and hips. Simple bodyweight exercises that your friendly physical therapist might recommend like side leg lifts and clamshells and glute extensions will help. Look ‘em up on YouTube.
Runners knee? Strengthen your quads, especially the VMO and roll out and loosen the muscles that lead to your IT Band.
Don’t rush to get that MRI unless you’ve had a nasty injury. Speak to your friendly Orthopedist first for a proper clinical evaluation. Seek out the root cause.
And now for the music:
Mr. Blue Sky is from ELO’s 1977 ‘Out of the Blue.’ Check out the end of the song to truly appreciate how ELO so masterfully blended rock with classical strings and opera. It will blow your mind.
PLEASE share this with friends, family, and even kind strangers you meet at Whole Foods. Who HASN’T had a wonky knee from time to time, right?
And a shout out and thank you to my buddy and med school roommate Dave for sharing great tunes and conversation along that winding desert road.

Oh and BTW, if you do roll out your quads with a foam roller, try to bend your knee as you roll. By engaging your hamstrings with the bend, you relax and elongate your quads. You’ll more easily find those knots and trigger points. When you find a sore spot, just hold that position and take 5 deep breaths and let the muscle melt in to the roller. Gently move around on the roller and you may find the knot disappear!
Well written! An enjoyable read as always.